

Blog
What Occupational Therapists Recommend for Dysphagia Management

Dysphagia can impact the bolus preparation, bolus propulsion, and the protection of the airway during the swallow. Occupational Therapists work with everyday routines that help to make eating safer, less strenuous and more dignified. There are ways to minimize coughing and throat clearing and get more food on the plate with practical changes, posture, pace and set up at mealtimes. Regular routines also enable families and staff to detect early changes such as an increase in meal times, a variation in voice or an increase in fatigue.
Types of Dysphagia
| Type | Common Symptoms | Common Causes |
|---|---|---|
| Esophageal Dysphagia | Difficulty swallowing, food stuck in the chest or throat, regurgitating, heartburn. | Acid reflux, narrowing of the esophagus, growths of the esophagus, and motility disorders |
| Oropharyngeal Dysphagia | Problems with swallowing, coughing or choking when eating and drinking, drooling, and weight loss. | Stroke, Parkinson’s, MS or other neurological conditions. |
Start With A Safety Check
Occupational therapists typically check alertness, breathing pattern, voice clarity and stamina before a tray is brought in to the patient. Recommendations are generally based on the speech therapy advice, as timing of the swallow and airway protection are the main factors that control risk. If a plan includes “thickened drinks” it is important to be consistent among all cups and caregivers. A standardized thickener (Simply Thick) will help to minimize unnecessary variation in flow rate throughout the day (at breakfast, lunch and the evening meal).
Positioning and Oral Care in Dysphagia Management
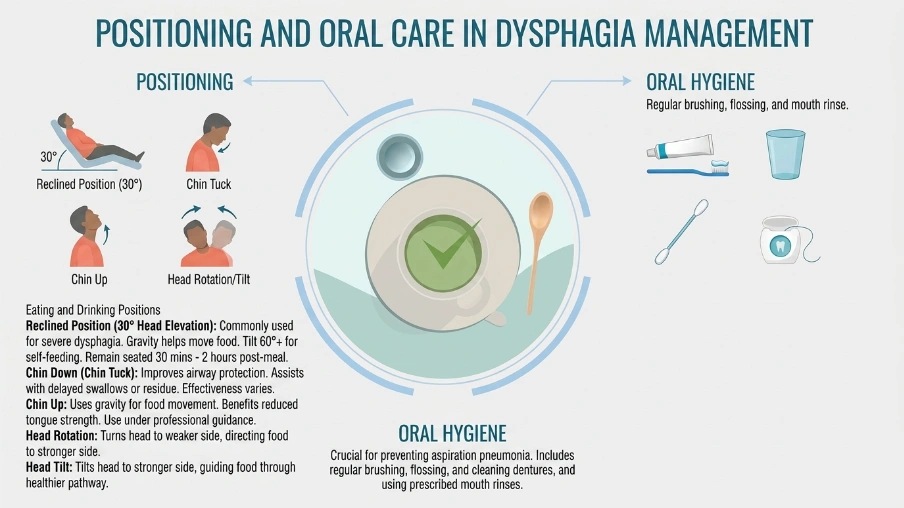
Positioning
Proper body posture plays an important role in safe swallowing. Adjusting a patient’s position can improve swallowing efficiency and reduce the risk of aspiration.
Eating and Drinking Positions
Reclined Position (30° Head Elevation)
- Commonly used for individuals with severe dysphagia.
- Gravity helps move food from the mouth to the throat.
- May reduce aspiration risk by supporting safer bolus movement.
- A tilt of 60° or more is usually needed for self-feeding.
- Remaining seated for 30 minutes to 2 hours after meals can help prevent reflux and aspiration.
Chin Down (Chin Tuck) Position
- Helps improve airway protection during swallowing.
- Can assist with delayed swallowing reflexes or food residue in the throat.
- Its effectiveness varies between individuals and should be assessed clinically.
Chin Up Position
- The head is tilted backward before swallowing.
- Uses gravity to assist food movement from the mouth.
- May benefit people with reduced tongue strength or prolonged oral transit time.
- Should only be used when throat and airway function are intact and under professional guidance.
Head Rotation
- Turning the head toward the weaker side directs food toward the stronger side.
- Useful for patients with one-sided pharyngeal weakness or paralysis.
Head Tilt
- Tilting the head toward the stronger side helps guide food through the healthier swallowing pathway.
Oral Hygiene
Good oral care is essential for people with dysphagia, as it lowers the risk of aspiration pneumonia caused by harmful bacteria entering the lungs.
Recommended Oral Care
- Brush teeth and oral tissues after meals and before bedtime.
- Keep the lips and mouth well hydrated.
- Use an antiseptic mouthwash twice daily, especially for individuals with severe dysphagia.
Free Water Protocol
Some patients with known aspiration may safely consume water under a supervised Free Water Protocol. However, eligibility should always be determined by a speech and language therapist.
Use Posture To Support Swallowing
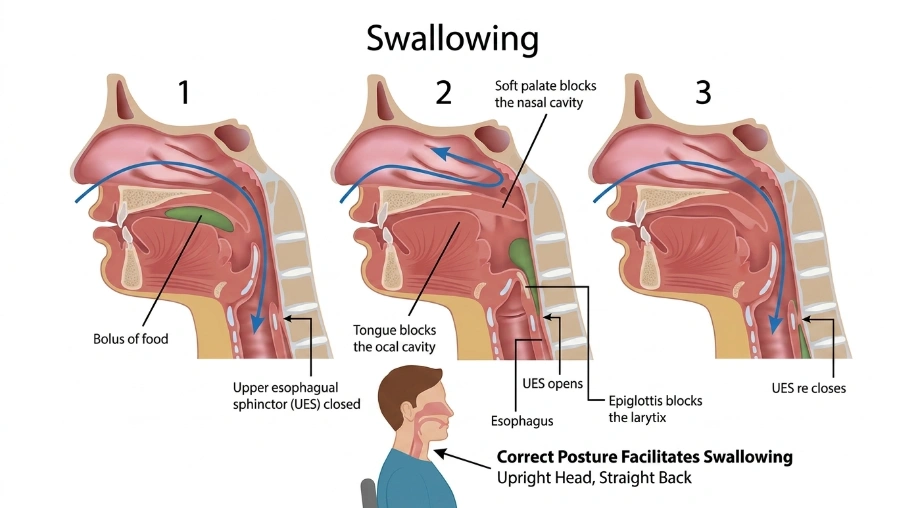
During feeding, sitting upright with back hips supported and feet on the floor helps to control the trunk. A small towel roll at the top of the back will help to minimize slumping. Head and neck position should be consistent with care plan, as this may involve a chin-down or head-turn positioning which is dependent on the assessment. Care partners can remind someone to get in line — but not to push them into it. Consistent placement of a chair or simple visual markers or a mirror can be used to reinforce a safe position.
Match Texture To Ability
Texture modifications provide a decreased risk when chewing abilities, tongue control, or timing of swallowing is compromised. Occupational therapists liaise with the team to ensure that the level of the meal, moisture and particle size, are all correct.
Premature spilling usually occurs with the mixed texture of broth with chunks. Dry crumbs may become scattered and cause sensitive tissue to become irritated. Using consistent steps in preparation, measuring recipes and using the same labels on the containers provide the same texture for each caregiver.
Pace Meals For Breathing
The swallowing must happen in synchrony with breathing and speed is important. Smaller bites, measured sips and planned pauses minimize any overfilling of the mouth and hasty breathing.
There are techniques taught by many therapists using a “set down” routine (where utensils are placed on the table between bites), or a simple timer to cue breaks. Risk is increased by fatigue and shorter meals with planned snacks can help. Look out for watery eyes, clearing the throat repeatedly, or a new “wet” voice.
Train Safe Self Feeding Skills
- Independence can enhance safety, when the individual is in control of the timing and of the size of the portions. Occupational Therapists use reach, grab and bring to mouth patterns with adaptations as necessary. Depending on the plan, a handled cup, two-hand support or straw limit may be recommended.
- Confusion can be limited by using visual cues, colour contrast plates and simplified place settings. Skill building can occur prior to meals, often decreasing pressure and increasing carryover.
Support Medication Swallowing
Tablets may be difficult to chew, particularly if your mouth is dry or you have limited use of your tongue. Occupational therapists liaise with nursing and pharmacy as there are some medications that cannot be crushed or divided.
Some like to take pills better in a smooth puree and others require different timing from meals. The position of the head and the technique of taking a sip should be in line with the swallow plan. Having a written medication routine helps to avoid missed doses and accidentally taking more.
Reduce Aspiration Risk During Daily Care
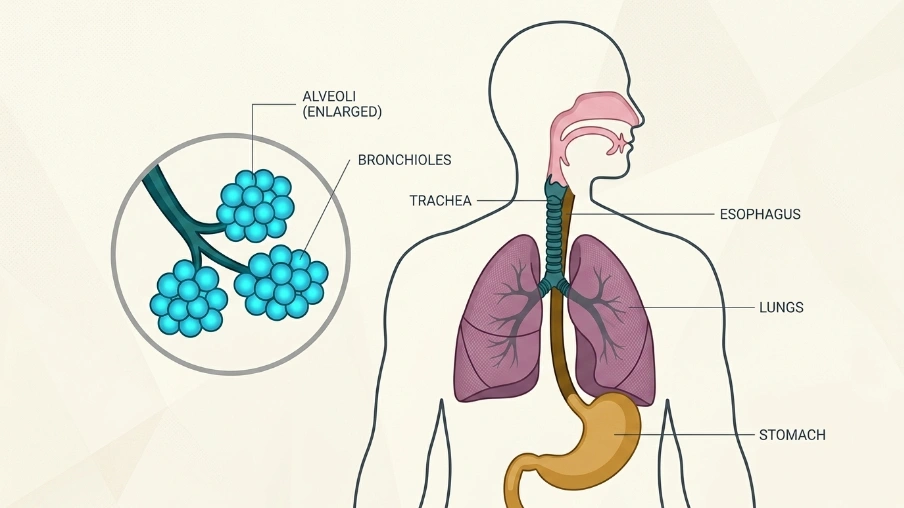
- Swallow safety extends beyond food and drinks. Oral hygiene, denture cleaning, and mouth moisture reduce bacterial load in the mouth, which matters if aspiration occurs.
- Therapists may recommend upright positioning for mouth care and suction readiness when indicated. Reflux management, meal timing, and avoiding heavy late intake can also help. Caregivers should report new fever, chest congestion, or repeated coughing after eating or drinking.
Watch For Changes And Escalate Early
Occupational therapists encourage tracking patterns rather than single incidents. Weight loss, longer mealtimes, new avoidance, and recurring respiratory illness can signal a change in swallow function.
A short checklist can capture fatigue, throat-clearing frequency, or appetite decline. Sudden shifts need prompt medical evaluation. Regular re-checks help ensure that texture levels and strategies still fit current abilities, health status, and personal goals.
Conclusion
Consistent routines are essential for effective dysphagia care to prevent choking and ensure nutrition and hydration. OTs will begin with posture, environment, pacing, and the proper assistive devices, and ultimately create a plan that can be implemented consistently by the caregiver. Tracking fatigue, intake and warning signs enables earlier fatigue adjustments to be made before setbacks. Many feel safer eating, less anxious and more involved in social eating with shared guidance and follow through.